
OF THE TYPE USED BY WALTER FREEMAN, M.D. , NEUROSURGEON AND LOBOTOMIST. MANUFACTURED TO HIS SPECIFICATIONS BY HENRY A. ATOR OF WASHINGTON, D.C.
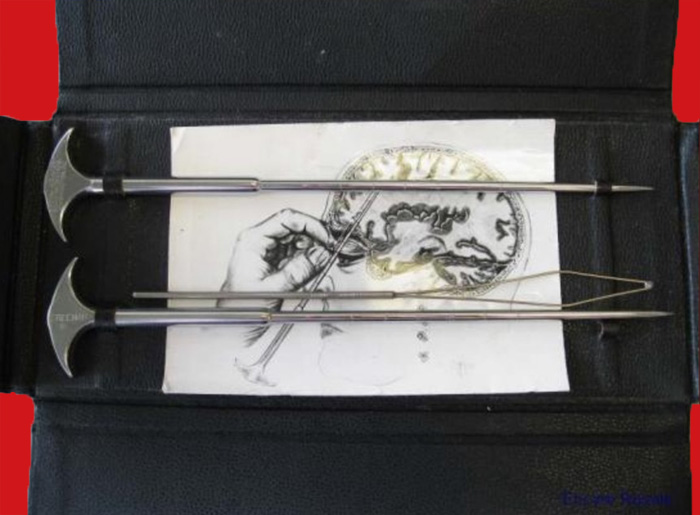
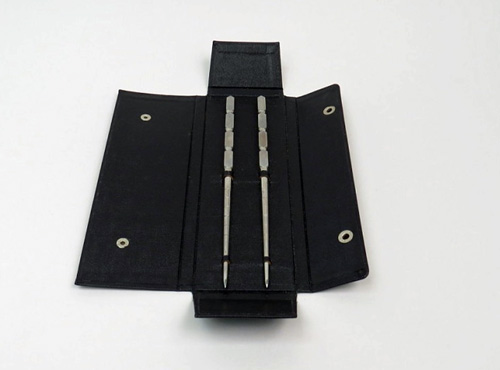
This is a rare example of an original lobotomy set with three instruments. It includes two orbitoclasts in the original case. A third instrument, possibly a form of leucotome, and a small paper sketch illustrating the procedure were found in the case.
THE LOBOTOMY INSTRUMENTS
Invented by Canadian neurosurgeon Dr. Kenneth G. McKenzie in the 1940s, the leucotome has a narrow shaft which is inserted into the brain through a hole in the skull, and then a plunger on the back of the leucotome is depressed to extend a wire loop or metal strip into the brain. The leucotome is then rotated, cutting a core of brain tissue. Although this instrument lacks a plunger, the handle pushes up to create the wire loop seen in the photograph. It may well be a simpler design, intended to achieve the same effect.
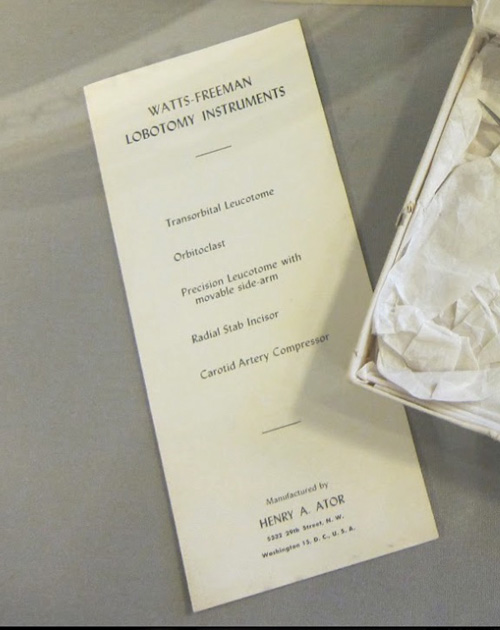
Lobotomy Instruments
(Note manufacturer – Henry A. Ator)
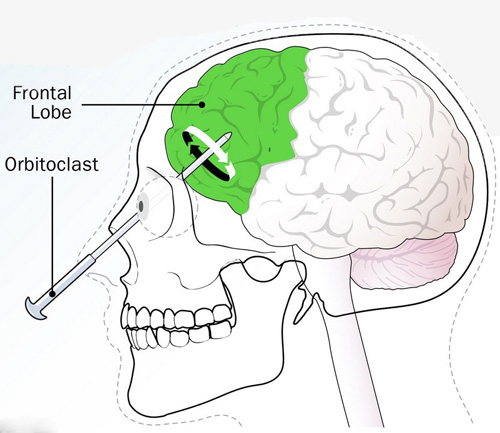
The orbitoclast was invented by Dr. Walter Freeman in 1948, used to replace the leucotome used up to that point for transorbital lobotomies. The instrument is, essentially, an ice pick with some gradation marks etched onto the shaft. The orbitoclast was inserted at the top of the eye-socket into the front of the brain, and then manipulated to sever neuronal connections (a more detailed explanation is given below). The leucotome occasionally broke off in the patient’s head, necessitating surgical removal, so Freeman commissioned Henry A. Ator to design a more durable and reliable replacement – and the orbitoclast was born. The website https://dcist.com/story/16/03/07/walter-freeman-lobotomy-st-elizabet/ states the following:
“The ice pick broke on more than one occasion, and Freeman commissioned Henry Ator, a Tenleytown machinist, to make him a new instrument, the orbitoclast. Some of Freeman’s very own surgical instruments, including a gruesome-looking ice pick, currently live in the archives at GWU.”
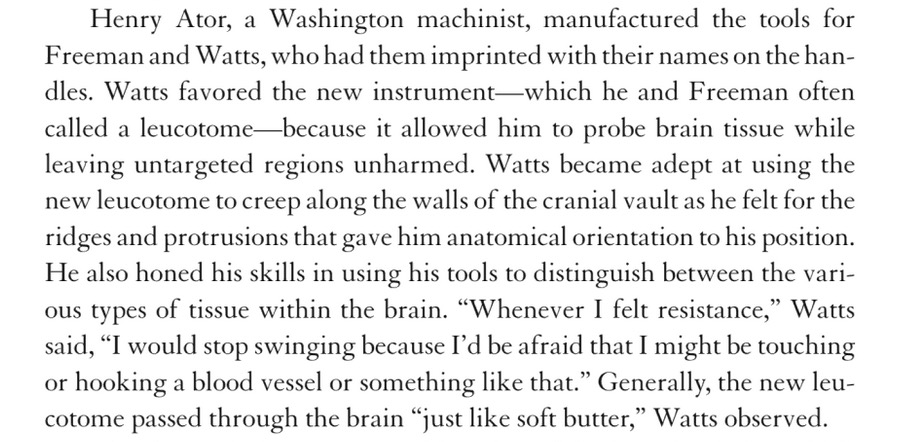
Another source confirming the Freeman-Watts-Ator connection is found on page 144 in the book “The Lobotomist: et.al. ” by Jack El-Hai:
HENRY A. ATOR , THE INSTRUMENT-MAKER
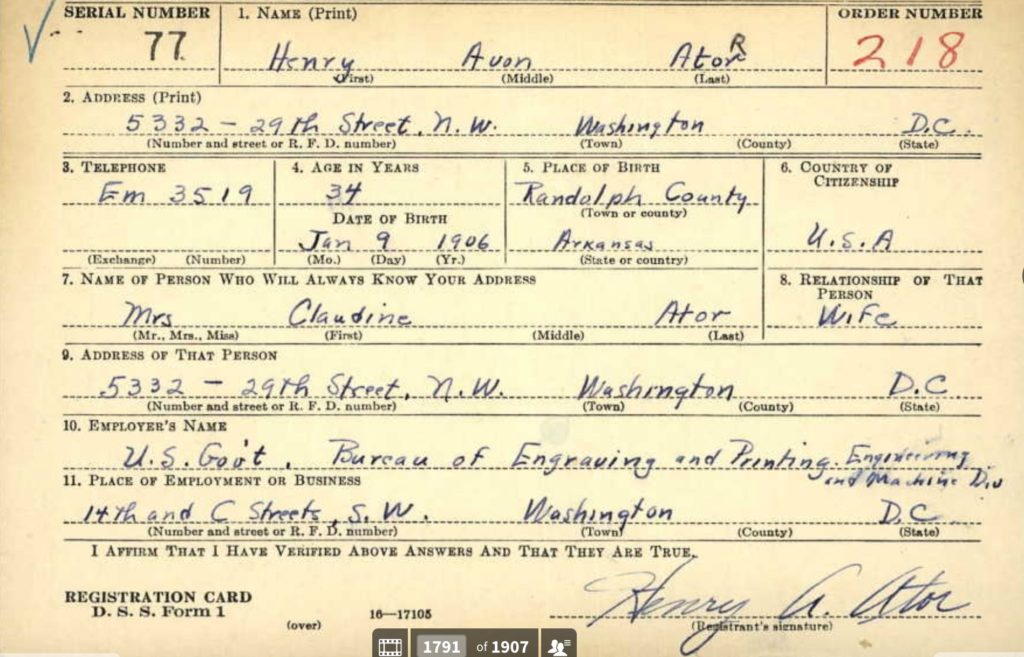
I was able to find some historical information about Henry Avon Ator. He was born in 1906 in Randolph county, Arkansas, had a 10th grade education, and married Claudine Caie in 1934. In 1940, he lived at 5332 29th St. NW in the District of Columbia, along with his wife and one-year-old son, Robert. His occupation is a “machinist” at the Bureau of Engraving and Printing, Engineering and Machine Division. Their only child, Col. Robert Avon Ator, died in 2017.
I am well aware that there are very good reproductions of orbitoclasts and other lobotomy instruments on the market. The one shown here was found at estate sale in Michigan, but no other history was available. One of the orbitoclasts is marked on one side of the handle with the following:
Mfd. by H.A. Ator
5332 29th St. N.W.
Washington, D.C
The other orbitoclast is marked “Freeman” on one side of the head. The instrument which I believe may be an earlier version of a wire-loop type pf leucotome is unmarked.
As noted previously, there are reproduction orbitoclasts in the market and they are invariably marked “Freeman”. There is a very good reason why I believe that the instruments shown here are original, along with the case. At the National Museum of American History at the Smithsonian Institute, there is one example of each of the instruments listed on Ator’s pamphlet shown previously. All were donated to the Smithsonian by Henry A. Ator himself.
The two cased instrument sets are shown below. The leatherette case of each is identical to the one in my collection.




Cased set of “Freeman Transorbital Leucotomes”
made by Henry A. Ator

(From page 135 of the book Psychiatry and Its Discontents
by Andrew Stull, Univ. of California Press, 2021)

The cases in the museum are a perfect match to the one shown in my collection, and the manufacturing stamp of Ator on the examples shown directly above is a perfect match as well.
Henry Avon Ator died at age 89 in 1995, and is buried alongside Claudine in Parklawn Memorial Park in Rockville, Maryland. There is a Masonic symbol on the gravestone:

THE LOBOTOMISTS
Dr. Walter J. Freeman attended Yale and the University of Pennsylvania School of Medicine, then studied neurology and psychiatry in Europe. He introduced insulin shock therapy and ECT for patients at George Washington University Hospital in Washington D.C., where he served on the faculty. He also had a private practice and was director of the laboratories at St Elizabeth’s Hospital. Reflecting on his time with the residents at “St. Es”, he wrote: “[They inspire] a weird mixture of fear, disgust and shame …” “The slouching figures, the vacant stare or averted eyes, the shabby clothing and footwear, the general untidiness—it all aroused rejection rather than sympathy or interest.” You, the reader, can draw your own conclusions as to his character.
Dr. James W. Watts attended the Virginia Military Institute and the University of Virginia School of Medicine. Watts is noteworthy for his professional partnership with the neurologist and psychiatrist Walter Freeman. The two became advocates and prolific practitioners of psychosurgery, specifically the lobotomy. Watts wrote two books on lobotomies with Dr. Freeman: “Psychosurgery, Intelligence, Emotion and Social Behavior Following Prefrontal Lobotomy for Medical Disorders” in 1942 and “Psychosurgery in the Treatment of Mental Disorders and Intractable Pain” in 1950.
MARKETING THE TRANSORBITAL LOBOTOMY
(WARNING – GRAPHIC TEXT)
The theory behind the lobotomy procedure is simply this: by severing the connections that the frontal lobes, or prefrontal cortex, have to the rest of the brain, they could calm patients’ emotions and stabilize their personalities without doing away with their intelligence and motor functions. But – theory does not always become reality.
Upon finding out that chimpanzees became subdued when their frontal lobes were damaged, and spurred into action by Portuguese neurologist Egas Moniz’ experiments on people, Freeman and Watts started practicing on brains from the hospital morgue, and in 1936 they were ready for their first patient, one Alice Hood Hammatt, a 63 year old housewife, who suffered from agitated depression and sleeplessness. The technique of entering the frontal lobes through the eye sockets was still far off into the future. Instead, they drilled six holes into the top of her skull. According to Freeman, Mrs. Hammett emerged transformed, able to “go to the theater and really enjoy the play … ” She lived another five years.
Ten years later, Freeman perfected a new method. Moniz’s technique required a patient to go under general anesthesia in an operating room. Freeman wanted to find a technique that was faster, more accessible and less expensive, so he decided to get to the prefrontal cortex through the eye sockets instead, and developed the procedure known as “transorbital lobotomy”. It was performed without anesthesia – Freeman used electroconvulsive “shock”treatment to induce a seizure, resulting in an unconscious state.
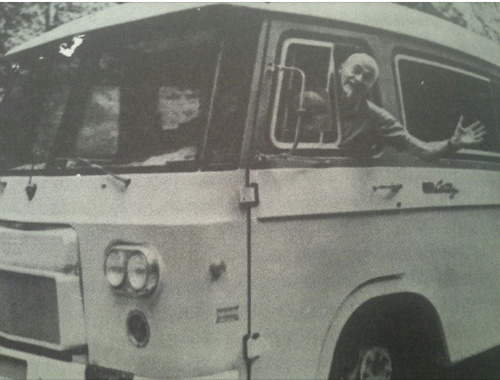
The procedure was also performed on people who were considered extremely emotional, difficult to handle or simply “moody.” Eventually, Freeman’s championing (i.e. marketing) of the procedure included a traveling “lobotomobile,” a customized van in which he demonstrated his technique to the press as well as doctors at mental hospitals (in fairness, there is no evidence that Freeman ever used the term “lobotomobile”.) He liked to show off by entering both eye sockets at one time with two different orbitoclasts. Critics likened Freeman to an evangelist for the cause, while supporters claimed that getting a lobotomy was as safe and easy as getting a filling at the dentist. When Howard Dully (see below) received the records of the lobotomy performed on him as a child, he discovered that it had cost his parents less than $200. The popularity of lobotomies spread like wildfire, with thousands of people being subjected to the 10-minute procedure.
Freeman had many critics among his medical colleagues. To one in particular, he had just gone too far. In 1950, Walter Freeman’s long-time partner James Watts left their practice and split from Freeman due to his opposition to the cruelty and overuse of the transorbital lobotomy.
Freeman promoted the procedure to more than 55 hospitals in 23 states. At AMA meetings, he set up graphic exhibits and used hand-held clackers to draw audiences. Perhaps not content without a circus-like atmosphere around his promotion, he complemented his theatrical approach to demonstrating surgery by sporting a cane, goatee, and a narrow-brimmed hat.
Maybe it’s too much information – but you can get an idea of the kind of man he was by this:
FACT: Freeman wore a gold ring, dangling from a chain around his neck. He’d found it stuck on the penis of a patient years earlier in Philadelphia. After filing it off, he’d preserved it and wore it as a bit of a badge of honor.

Freeman charged just $25 for each procedure he performed, which made it within the reach of hundreds of people dissatisfied with the behavior of their mother. Or daughter. Or father. Or son. After all, it was like having an irritating tooth pulled… right?
Freeman kept records of 3,439 lobotomies he performed over his long career, most as an outpatient (office) procedure. He diligently kept a journal, recording his work in words and images, sometimes logging more than two dozen lobotomies in a single day. In a stretch of August 1958 entries, he journeyed from Nebraska, to Missouri, and then Iowa—50 transorbital lobotomies in just more than 4 days across 650 miles of America’s heartland.
Institutions jumped on the bandwagon, too. Lobotomies made difficult patients compliant, which helped to clear overcrowded hospitals, and unlike other psychiatric care, it promised immediate results. During its heyday in the 1940s and ’50s, the lobotomy was performed on some 40,000 patients in the United States, and on around 10,000 in Western Europe.
THE LOBOTOMY OPERATION – FACT AND FICTION
(WARNING – GRAPHIC TEXT AND PHOTOS FROM HERE ON!)
FACT: The procedure took 10 minutes… with no anesthesia – however, patients were rendered unconscious via electroshock therapy.

FACT: The large majority of lobotomy recipients in the U.S. were women.
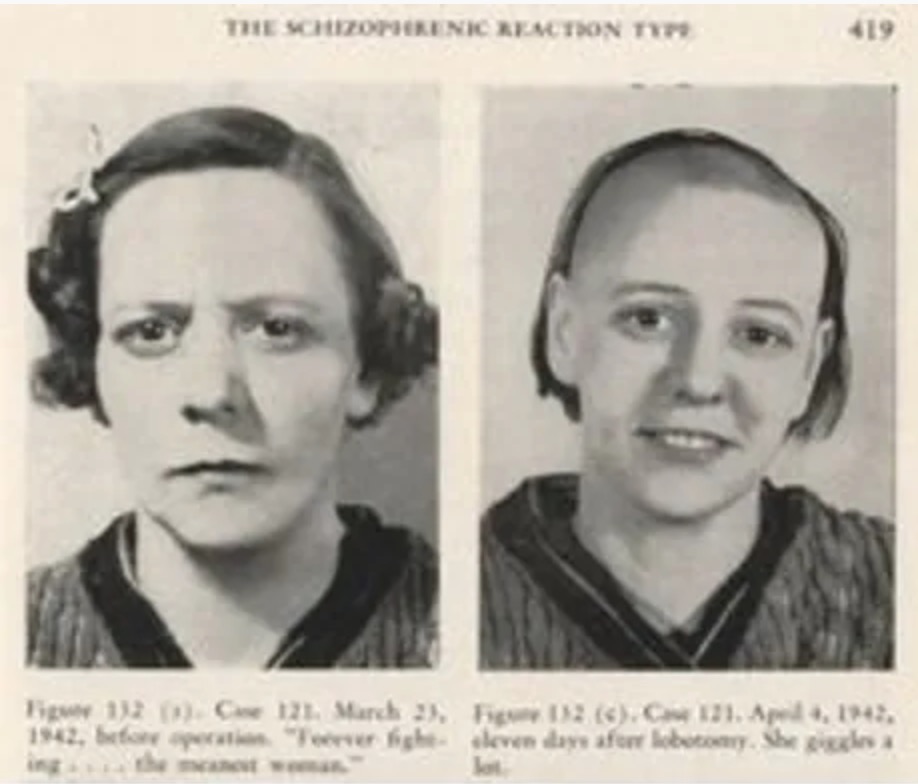
Freeman’s notes (at GWU) contain this misogynistic pearl: “Entranced by voices, this lady came down to earth and went back to keeping house,” reads a caption under a photo of one of his patients. “Simple schizophrenic patients become household pets after operation,” reads another.
In the early 2000’s, an article on Freeman in the Washington Post published a succinct, if lurid, contemporary description of a transorbital lobotomy:
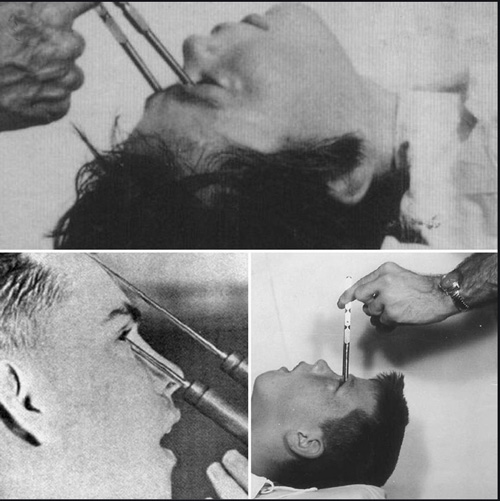
Walter Freeman lifted the patient’s eyelid and inserted an ice pick-like instrument called a leucotome through a tear duct. A few taps with a surgical hammer breached the bone. Freeman took a position behind the patient’s head, pushed the leucotome about an inch and a half into the frontal lobe of the patient’s brain, and moved the sharp tip back and forth. Then he repeated the process with the other eye socket.
Freeman observed that the bone at the back of the eye-socket was thin, and easily breached with the leucotome (later, orbitoclast). Just behind this fragile, bony wall lay the frontal lobes of the brain, responsible for executive functions like attention, reasoning, judgment, problem solving, creativity, emotional regulation, and impulse control. Literally scrambling this area with his pick-like tool, Freeman severed the neural connections between the anterior frontal lobes with the rest of the brain – think of all the information lost by cutting a fiberoptic cable carrying millions of bits of data, and you get the picture – a blank TV screen.
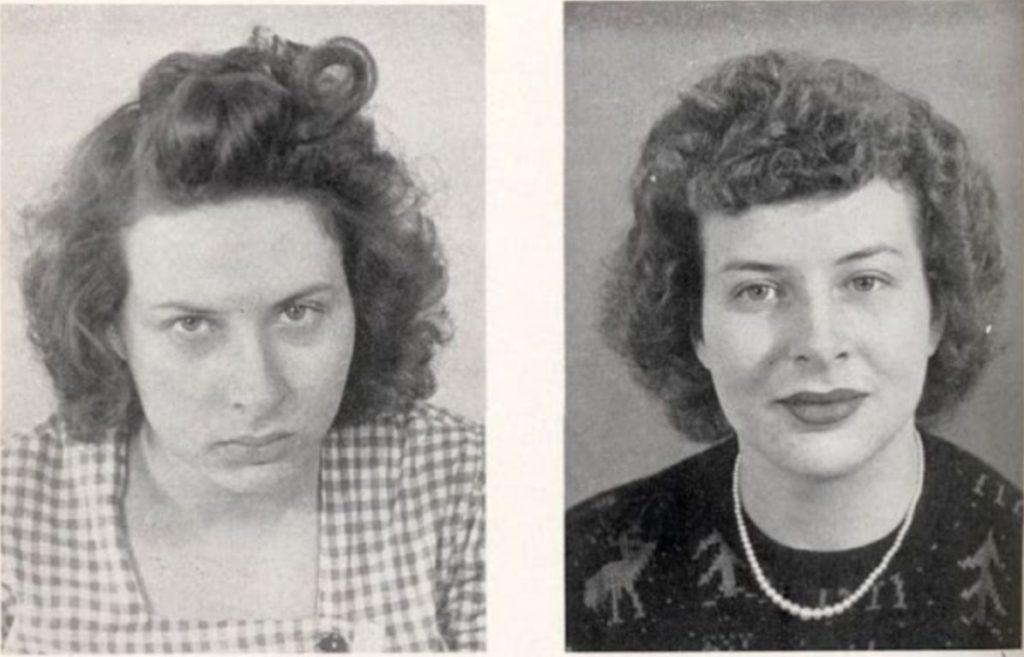
One of the biggest tragedies was that people were kept in the dark about the horrific consequences. Before-and-after photos were publicly circulated, showing either a very depressed, or manic-looking person followed by a photo of the same person looking calm, or even smiling. Not infrequently, the photographs portrayed the “before” example as a depressed, disheveled woman/wife, who in the “after” photo turned, Cinderella-like, into a picture-perfect example of the happy housewife, complete with hairdo, stylish clothes, and makeup:

Few people realized that, in the “after” picture, the patient was often more zombie than human:

Before: “Destructive…tore her clothes in threads…
After: “Returned to her habit of smashing toys…”
FACT: Freeman performed the procedure despite the fact that he had no formal surgical training. He wore neither mask nor gloves during the operation.
Freeman and Watts claimed 52 percent of their first 623 surgeries yielded “good” results, but they did not offer a clinical yardstick for what constituted an improvement. Patients often had to be retaught how to eat and use the bathroom. Relapses were common, some never recovered, and about 15% died from the procedure.
In 1951, during his promotional jaunt through the Midwest, one patient at Iowa’s Cherokee Mental Health Institute died when Freeman suddenly stopped for a photo during the procedure, and the surgical instrument accidentally penetrated too far into the patient’s brain.
Sadly, the most famous Freeman-Watts failure was JFK’s sister, Rosemary Kennedy. In her early young adult years, she experienced seizures and violent mood swings. Fearing she might one day bring embarrassment to the family, her father arranged a prefrontal lobotomy for her in 1941 when she was 23 years of age. While Watts used a slender, metal instrument to remove small areas of brain tissue, Freeman monitored Rosemary’s mental state, asking her to count backwards from ten or sing a favorite song. Watts cut away until Kennedy became unresponsive. The procedure left her permanently incapacitated, the mental equivalent of a two-year old, and rendered her unable to speak intelligibly. She was institutionalized and needed full-time care for 64 years, until she quietly passed away in a Wisconsin nursing facility in 2005.
THE CASE OF HOWARD DULLY
FACT: Freeman lobotomized nineteen minors, the youngest was a four-year-old child.
One of those minors was Howard Dully, who was lobotomized by Freeman as a 12-year-old boy in 1960. He wasn’t mentally ill; his stepmother wanted to change his personality, which she described as defiant. Dully wasn’t told about the operation until afterward. He states that “the surgery damaged me in many ways. But it didn’t ‘fix’ me, or turn me into a robot. So my family put me into an institution”. Dully claims that he always felt different, like “a freak” and “ashamed.” He lived in institutions for 10 years and battle addictions until his 50s.
After such a long (and needless) life struggle, Dully became sober and obtained a college degree in computer information systems; he became a California state certified behind-the-wheel instructor for a school bus company in San Jose, California.
In his 50s, with the assistance of National Public Radio producer David Isay, Dully started to research what had happened to him as a child. By this time, both his stepmother and Dr. Freeman were dead, and due to the aftereffects of the surgery, he was unable to rely on his own memories. He traveled the country with Isay and Piya Kochhar, speaking with members of his family, relatives of other lobotomy patients, and relatives of Dr. Freeman, and also gaining access to Freeman’s archives. On November 16, 2005, Isay broadcast Dully’s search as a Sound Portraits documentary on NPR.
In 2007, Dully published My Lobotomy, a memoir co-authored by Charles Fleming. The memoir relates Dully’s experiences as a child, the effect of the procedure on his life, and his efforts as an adult to discover why the medically unnecessary procedure was performed on him and the effect of the radio broadcast on his life. The book was positively received, with one critic calling it “harrowing”, “one of the saddest stories you’ll ever read”, and another “a forceful account of his survival” that “sheds light on the man who subjected him to one of the most brutal surgical procedures in medical history.”
Dully is (as of 2021) 72 years of age, and lives in Oakland, California. He is a true survivor.
THE END (SADLY, TOO LATE)
In 1967, Freeman performed a lobotomy on one of his original patients in Berkeley, California. It was her third lobotomy – Freeman believed in trying until he got it right. He severed a blood vessel, and the patient died from a brain hemorrhage three days later. Following this, Freeman was banned from operating. He continued to visit his former patients and tout the success of the procedure. During the last five years of his life, he performed no more lobotomies. He died from complications following an operation for cancer in 1972, at age 76.
In 1950, a drug named chlorpromazine (sold as Thorazine) was synthesized. This marked the beginning of the end for lobotomies as treatment for mental illness in the United States. Thorazine was the first in a series of anti-psychotic drugs, and some have described it as the biggest single advance in the treatment of schizophrenia – on par with what the discovery of penicillin did for the treatment of infectious diseases.
Although the lobotomy has been banned in several countries, it is still performed in limited numbers in several countries today. Often it is used to treat epilepsy. Now known as NMD (neurosurgery for mental disorder), lobotomies are performed in two hospitals in Great Britain as a last resort to treat obsessive-compulsive disorder and severe depression. Those who support it still believe it can be beneficial when all other treatments have failed.
In 2008, the FDA approved deep brain stimulation (DBS) for OCD, and the surgery is being investigated for depression. The surgery, which was developed for treating Parkinsons, involves inserting an electronic lead into the folds of the brain. Unlike lobotomies and surgeries such as capsulotomies, no surgical incisions are made. Nothing is severed. DBS for psychiatric illness is extremely rare and is used as a last resort.
In 1949, at Freeman’s urging, Moniz received the Nobel Prize. As Nassir Ghaemi MD of Tufts University in a review commented:
It is quite ironic that in that same year, the Australian psychiatrist John Cade would discover lithium … yet after the Moniz fiasco, the Nobel committee apparently has shied away from giving awards for direct treatment of mental illness, and thus the discoverers of lithium, antipsychotics, and antidepressants have never been duly recognized.
(some of the text was taken from author John McManamy http://www.mcmanweb.com/lobotomy.html)