
(AND THREE TALES ABOUT “CELEBRITIES” THAT WERE BLED)
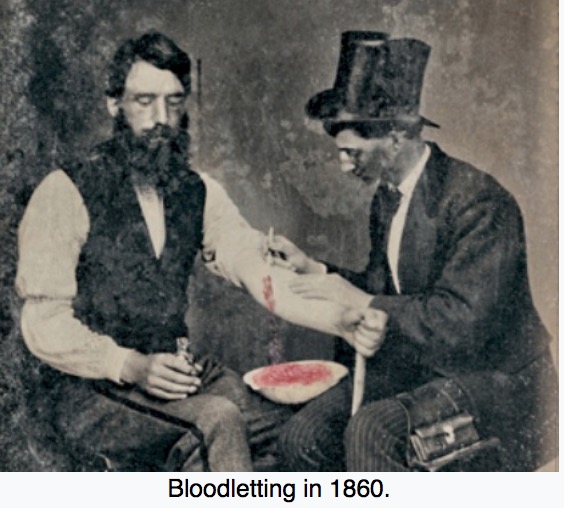
As far back as 400 BCE, Herodotus records that both bleeding and cupping were already used by the Egyptians. The Roman physician Galen wrote enthusiastically about the practice of bloodletting. He based his thinking on the humoral concept of disease, developed by the Hippocrateans. According to this theory, a person was healthy as long as the four humours (blood, phlegm, yellow bile and black bile) were in balance. Disease was the result of too much or too little of one of more of the humors. Galen held that fevers and inflammation were the result of an excess of one of the humors – usually blood. The best treatment for these condition, obviously, was bloodletting. Bloodletting was accomplished by the use of leeches, or by venesection (or as we call it, phlebotomy). Venesection is literally the process of cutting a vein to release blood, which would then be collected in a bowl.
Prior to Galen’s time, bloodletting tools were crude – fish teeth, or a sharpened stone. By Galen’s time, the “phlebotome” (a straight-bladed instrument with sharpened point) was used. Use of the phlebotome continued through the Middle Ages (when it was used to treat conditions such as the plague, smallpox, epilepsy and gout), up to the 15th century, when a new tool, the thumb lancet, was developed. The thumb lancet was adjustable, allowing for a more precise incision.
The practice reached its greatest popularity in the eighteenth and early nineteenth centuries. Popularity spurred innovation, and in the first quarter of the 1700s, both the spring lancet (which incised without using manual pressure, and allowed for depth control), and scarificator (a square box with multiple parallel rows of 8 – 12 tiny blades) were developed. Use of the scarificator obviated the need for multiple cuts with the lancet, and also allowed for control of the depth of the incisions. Leeches became especially popular in the early nineteenth century.
Bloodletting during this time was the standard treatment for fevers, as was used to treat a litany of other ailments. One British medical text recommended bloodletting for acne, asthma, cancer, cholera, coma, convulsions, diabetes, epilepsy, gangrene, gout, herpes, indigestion, insanity, jaundice, leprosy, ophthalmia, plague, pneumonia, scurvy, smallpox, stroke, tetanus, tuberculosis, and for some one hundred other diseases. Bloodletting was even used to treat most forms of hemorrhaging such as nosebleed, excessive menstruation, or hemorrhoidal bleeding. Before surgery or at the onset of childbirth, blood was removed to prevent inflammation (see Marie Antoinette’s case below!) Before amputation, it was customary to remove a quantity of blood equal to the amount believed to circulate in the limb that was to be removed.
The quantity of blood removed from any given patient depended on their diagnosis and clinical appearance – and was often massive. One often-used guideline was to bleed a patient to the point of fainting. One particular case in 1824 involved a French soldier who was stabbed in the chest and fainted from loss of blood. He was immediately bled 2/3’s of a quart “to prevent inflammation”. Over the subsequent month, he was bled a total of 6 liters of blood – more than all of the blood circulating in the body! He survived.
One reason for the continued popularity of bloodletting (and purging) was that, while anatomical knowledge, surgical and diagnostic skills increased tremendously in Europe from the 17th century, the key to curing disease remained elusive, and the underlying belief was that it was better to give any treatment than nothing at all. The psychological benefit of bloodletting to the patient may sometimes have outweighed the physiological problems it caused. Over time, the practice became more and more controversial, and slowly and steadily fell out of favor, as scientific studies and a change in beliefs about the cause of disease eclipsed the old way of thinking. It was outright banned in some countries. Nevertheless, it persisted even into the 20th century, with notable physicians such as Sir William Osler continuing to recommend it as an orthodox practice. There are but few medical indications today for therapeutic phlebotomy (and lancets and leeches are not used!). One condition is “hemochromatosis”, an inheritable condition in which the body stores too much iron, and can cause damage to the heart, liver, and pancreas.
THREE FAMOUS CASES OF BLOODLETTING
(AND NOT ALL WERE FATAL)
KING CHARLES II (1630 – 1685)

Aside from being famous for his spaniels, Charles suffered from chronic gout (too much “rich food”, just like Henry VIII. ) The gout may have been the reason he was plagued by an ulcer on his heel. For whatever reason, he awakened the morning of Monday, February 2, 1685 in great pain. He “gave ‘the dreadfulest shriek’ and developed convulsions, pallor and speechlessness.” His personal physician had just the remedy. He quickly slashed open a vein in the king’s left arm and filled a basin with about a pint of royal blood. Over the next few days, the king would be tortured by a swarm of physicians buzzing around his bedside. Later that day, they bled him again. They cupped him, scarified him, and blistered him, they gave him emetics, cathartics, and enemas. When he had another seizure the following day, they repeated the “therapy”. By the third day, he appeared to be stable, so was “just” given more powders, herbs and spices, and – “spirit of human skull”. The next day, Friday February 6, was his last. He apologized to his doctors for taking “an unconscionable time dying”, and confessed that “I have suffered very much, and more than any of you can imagine. My business will shortly be done”. He asked to see the light of the rising sun, after which he became acutely breathless and was bled another 12 oz. His speech failed, he became unconscious, and he died just before noon.
Post-mortem findings included cerebral edema (swelling of the brain), and the lungs, liver, kidneys and spleen were engorged with blood. One current physician who reviewed the case in detail, has proffered a most reasonable series of events which could have resulted in his death: chronic gout caused a foot ulcer and kidney damage, which caused uremic poisoning, which caused convulsions and swelling of the brain. The uremic poisoning was worsened by dehydration brought on by the bleeding, purgatives, and emetics, and ultimately resulted in his death. He concluded the following: “It is likely that Charles died from problems that his physicians at that time could not have cured, even had they known what they were and what caused them. However, it is equally likely that they hastened the end when it came.”
MARIE-ANTOINETTE (1755 – 1793)

At Versailles, not only the Queen, but princesses of the royal blood were required to give birth in public. Why? To prevent any substitution of the infant in case he was destined to reign. I say “he” by design, because France’s unwritten constitution prevented women to step unto the throne in their own right, though they could, and often did govern the Kingdom as Regents.
In the case of Marie-Antoinette, her first laying-in was all the more eagerly awaited since she had been married for eight years without presenting Louis XVI with an heir. For a Queen, this was a glaring failure. If she did not give birth to a male child (a Dauphin) her husband’s brother, who was the greatest enemy of the royal couple, would eventually ascend to the throne.
Her labor started on the morning of December 19th, 1778. The etiquette of the time was taken to such an extreme that her bedchamber was quickly filled with a motley crowd waiting to see the delivery. The room was so crowded, that one could hardly move around. Two chimney-sweeps climbed up on the furniture to get a better sight of the Queen.
Whether it was from the pain of labor, or the body heat created by the crowd, or the pressure to give birth to a boy, Marie-Antoinette fainted. And the child turned out to be a girl. Maybe the disappointment was enough to make the Queen lose consciousness.
The obstetrician decided that the patient needed to be bled, and more sensibly by modern standards, he called for the windows to be opened wide. Louis XVI sprang to action and rushed to open the windows. The Court’s head surgeon then seized his lancet and bled the Queen. Whether thanks to his ministrations, or more likely the rush of fresh air in the stifling room, she opened her eyes.
The 18th century ushered in new and improved bloodletting devices, as well as another bloodletting device (of sorts) – the guillotine. When Marie-Antoinette died on October 16, 1973, fifteen years after that birth, it was – technically speaking, not from loss of blood. As we are all aware, it was from loss of her head.
And her husband’s brother became Louis XVIII.
GEORGE WASHINGTON (1732 – 1799)
We have all heard the story how George Washington was “bled to death”. Yes, it is true that after he became acutely ill, he was bled – a lot– and suffered horribly in his final hours. Equally true is that his physicians did the best they could, considering the now-discredited medical theories and therapeutics of the time. Bloodletting was in and of itself not the cause of his death. Was it is contributing factor? Maybe. But Dr. David Morels, who has thoroughly researched the subject, believes that the amount of blood lost, while considerable, would not likely kill a man of his size.
There is so much material on the subject of his death, it would be a struggle to research the case from beginning to end and piece it together in a relatively concise fashion.
The short version is this:
Two days before he died, an apparently healthy Washington went out for a ride on a cold, miserable day. He decided to stay in his wet clothes so he could be on time for dinner.
That night, Washington woke his wife Martha to say he was feeling very sick, and that he could hardly breathe or talk on his own. The former President asked his overseer, Albin Rawlins, to bleed him. Doctors then arrived and bled him four more times over the next eight hours, with a total blood loss of 40 percent.
Washington also gargled with a mixture of molasses, vinegar and butter; he inhaled a steam of vinegar and hot water; and his throat also was swabbed with a salve and a preparation of dried beetles. An enema was also used. By late afternoon, Washington knew he was dying and asked for his will.
On December 14, 1799, George Washington died at his home after a brief illness and after losing about 40 percent of his blood. Many theories as to his diagnosis have floated around over the years; one that explains all of his symptoms is “acute bacterial epiglottis”. Not everyone agrees with that theory, with inflammatory quinsy, or a peritonsillar abscess, as another possible killer.
The long version is better for those medical people interested in a “blow by blow” account of the case. I have shamelessly reproduced most of an excellent article titled “Dec. 14, 1799: The Excruciating Final Hours of President George Washington” written by Dr. Howard Markel, which appeared in the “Health” section of the online PBS News Hour on December 14, 2014. It can be found here: https://www.pbs.org/newshour/health/dec-14-1799-excruciating-final-hours-president-george-washington
American history buffs know so much about George Washington’s final illness because of a wealth of primary source documents as well as the herculean efforts of Dr. David Morens, an epidemiologist and the Senior Advisor to the Director of the National Institute for Allergy and Infectious Diseases. Dr. Morens wrote about these harrowing last hours for the New England Journal of Medicine in 1999. (1999; 341: 1845-1849). Another fascinating account of Washington’s medical history can be found in a 1933 issue of the Bulletin of the Institute of the History of Medicine written by Dr. J.H. Mason Knox Jr. (1933; 1: 174-191). And even more intriguing is a long letter about Washington’s last illness, written by Col. Tobias as the events unfolded.
Here is the article:
“It was a house call no physician would relish. On Dec. 14, 1799, three doctors were summoned to Mount Vernon in Fairfax County, Va., to attend to a critically ill, 67-year-old man who happened to be known as “the father of our country.”
On the afternoon of Dec. 13, a little more than 30 months into his retirement, George Washington complained about a cough, a runny nose and a distinct hoarseness of voice. He had spent most of the day on horseback in the frigid rain, snow and hail, supervising activities on his estate. Late for dinner and proud of his punctuality, Washington remained in his damp clothes throughout the meal.
By 2 a.m. the following morning, Washington awoke clutching his chest with a profound shortness of breath. His wife Martha wanted to seek help but Washington was more concerned about her health as she had only recently recovered from a cold herself. Washington simply did not want her leaving the fire-warmed bedroom for the damp, cold outside. Nevertheless, Martha asked her husband’s chief aide, Col. Tobias Lear, to come into the room. Seeing how ill the general was, Col. Tobias immediately sent for Dr. James Craik, who had been Washington’s physician for more than 40 years, and the estate’s overseer, George Rawlins, who was well practiced in the art of bloodletting.
Only a few hours later, 6 a.m., Washington developed a pronounced fever. His throat was raw with pain and his breathing became even more labored.
At 7:30 a.m., Rawlins removed 12 to 14 ounces of blood, after which Washington requested that he remove still more. Following the procedure, Col. Lear gave the patient a tonic of molasses, butter and vinegar, which nearly choked Washington to death, so inflamed were the beefy-red tissues of his infected throat.
Dr. Craik entered Washington’s bedchamber at 9 a.m. After taking the medical history, he applied a painful “blister of cantharides,” better known as “Spanish fly,” to Washington’s throat. The idea behind this tortuous treatment was based on a humoral notion of medicine dating back to antiquity called “counter-irritation.” The blisters raised by this toxic stuff would supposedly draw out the deadly humors causing the General’s throat inflammation.
At 9:30 a.m., another bloodletting of 18 ounces was performed followed by a similar withdrawal at 11 a.m. At noon, an enema was administered. Attempts at gargling with a sage tea, laced with vinegar were unsuccessful but Washington was still strong enough to walk about his bedroom for a bit and to sit upright in an easy chair for a few hours. His real challenge was breathing once he returned to lying flat on his back in bed.
Dr. Craik ordered another bleeding. This time, 32 ounces were removed even though Elisha Cullen Dick, the second physician to arrive at Mount Vernon, objected to such a heroic measure. A third doctor, Gustavus Richard Brown, made it to the mansion at 4 p.m. He suggested a dose of calomel (mercurous chloride) and a tartar emetic (antimony potassium tartrate), guaranteed to make the former president vomit with a vengeance.
After the fourth bloodletting, Washington appeared to rally somewhat. At 5 p.m., he was having an easier time swallowing and even had the energy to examine his last will and testament with Martha. Soon enough, he was again struggling for air. He told Dr. Craik: “Doctor, I die hard; but I am not afraid to go; I believed from my first attack that I should not survive it; my breath can not last long.” Ever the gentleman, even in extremis, the General made a point of thanking all three doctors for their help.
By 8 p.m., blisters of cantharides were applied to his feet, arms and legs while wheat poultices were placed upon his throat with little improvement. At 10 p.m., Washington murmured some last words about burial instructions to Col. Lear. Twenty minutes later, Col. Lears’ notes record, the former president settled back in his bed and calmly took his pulse. At the very end, Washington’s fingers dropped off his wrist and the first president of our great Republic took his final breath. At the bedside were Martha Washington, his doctor, James Craik, Tobias Lear, his valet, Christopher Sheels, and three slave housemaids named Caroline, Molly and Charlotte.
Washington’s physicians, as doctors are wont to do, argued heatedly over the precise cause of death. Dr. Craik insisted that it was “inflammatory quinsy,” or peritonsillar abscess. Dr. Dick rejected such a possibility and offered three alternative diagnoses: stridular suffocatis (a blockage of the throat or larynx), laryngea (inflammation and suppuration of the larynx), or cynanche trachealis. The last arcane medical diagnosis (from the Latin, for “dog strangulation”), which prevailed as the accepted cause of Washington’s death for some time, referred to an inflammation and swelling of the glottis, larynx and upper trachea severe enough to obstruct the airway.c
Washington’s physicians, as doctors are wont to do, argued heatedly over the precise cause of death. Dr. Craik insisted that it was “inflammatory quinsy,” or peritonsillar abscess. Dr. Dick rejected such a possibility and offered three alternative diagnoses: stridular suffocatis (a blockage of the throat or larynx), laryngea (inflammation and suppuration of the larynx), or cynanche trachealis. The last arcane medical diagnosis (from the Latin, for “dog strangulation”), which prevailed as the accepted cause of Washington’s death for some time, referred to an inflammation and swelling of the glottis, larynx and upper trachea severe enough to obstruct the airway.
Back in 1799, Washington’s physicians justified the removal of more than 80 ounces of his blood (2.365 liters or 40 percent of his total blood volume) over a 12-hour period in order to reduce the massive inflammation of his windpipe and constrict the blood vessels in the region. Theories of humoralism and inflammation aside, this massive blood loss — along with the accompanying dehydration, electrolyte imbalance, and viscous blood flow — could not have helped the president’s dire condition.
A fourth physician, William Thornton (who also designed the U.S. Capitol building), arrived after Washington succumbed. Thornton had expertise in the tracheotomy procedure, an extremely rare operation at the time that was performed only in emergencies and with occasional success. Dr. Dick, too, advocated this procedure — rather than the massive bloodletting — but given the primitive nature of surgical science in 1799, it is doubtful it would have helped much.
In the 215 years since Washington died, several retrospective diagnoses have been offered ranging from croup, quinsy, Ludwig’s angina, Vincent’s angina, diphtheria, and streptococcal throat infection to acute pneumonia. But Dr. Morens’s suggestion of acute bacterial epiglottitis seems most likely. In the end, we will never really know, which constitutes half of the fun enjoyed by doctors who argue over the final illnesses of historical figures.“